

Covid-19 – a case for medical detectives
WOLFGANG WODARG, 2. Mai 2020, 0 Kommentare, PDFNote: This article is also available in German, Portuguese, French and Turkish.
Before I describe my research on these findings which are very disturbing to me, I would like to say a few words about the assessment of the corona crisis, the reliability of the SARS-CoV-2 PCR test, as well as ubiquitous fear and how it is used politically.
In my investigations into the events after Wuhan, which have completely changed the world since the beginning of 2020, I realized quickly that although we are experiencing a new Corona virus variant, it does not – in view of German data on mortality and morbidity – differ significantly from what has been, or could have been, observed in recent years.
Corona viruses have not been the focus of epidemiological surveillance worldwide, as they have not contributed significantly to globalised seasonal respiratory viral infections, except in the short term in China (SARS 2002/2003) and in the Arab countries (MERS from 2012). There were also no existing vaccines that could have been recombined and marketed annually, as is the case for influenza.
As is well known, regular global episodes of flu have been referred to as "pandemics" since the swine flu of 2009, in an inflationary manner and focusing on single pathogens. In this context, vigilance and historically justified mistrust have long been required. For if our normal, changing and globally circulating viral winter guests, such as the H1N1 viruses in 2009, already meet the criteria of a pandemic, then the term has become meaningless. Before 2009, things were different. At that time, the necessary characteristics of a pandemic included a great many serious illnesses and numerous deaths, with a worldwide catastrophic overload of health care.
To me the sole infection epidemiological aspects of the Wuhan phenomenon are clearly laid out by and large. According to the available figures of the German networks for the surveillance of acute respiratory infections (ARI), the Influenza consortium and the Flu Web, and according to hospital data for ARI, as well as data on the utilization of intensive care units in the country, the flu wave 2019/2020 with its diverse pathogen spectrum has passed without any particularities. Only the consultations in the reporting wards apparently took place much less frequently in the last weeks of the season due to the lockdown.
With regard to acute seasonal respiratory diseases there is currently no reason to fear increased acute respiratory infections. From a medical point of view and considering the available data special precautions are now unnecessary – even if the government says otherwise.
The SARS-CoV-2 PCR test: non-specific, medically useless, but anxiety-producing
Because of the great importance for the Covid-19 occurrence, special attention must be paid to the SARS-CoV-2 PCR test – the only instrument available to measure the virus and to be able to talk about a new spread at all. My assessment on this has not changed since the end of February: Without the PCR test for SARS-CoV-2 viruses designed by German scientists, we would not have noticed a corona "epidemic" or even a "pandemic".
After the WHO recommended it ("not for medical diagnostic purposes"), the test was used all over the country in the attempt to find fragments of SARS virus. An institution in China, whose name was not mentioned by one of the developers of the PCR test, Prof. Drosten, during an interview on German public radio “Deutschlandfunk”, confirmed to the virologist that the test used by him found the SARS fragment they were looking for in the Wuhan SARS virus.
My assessment of this test which is not officially accredited and not approved for medical purposes and now used to search for "cases" worldwide, is as follows:
How can a test that turns out positive for the many different SARS viruses of bats, dogs, tigers, lions, domestic cats and humans, which have been changing and spreading worldwide for many years, be called specific for the detection of an allegedly only four-month-old SARS-CoV-2?
Apparently it is a sensitive test that produces too many positive results. Therefore it can also detect many – in the meantime naturally recombined – SARS-like pathogens. This does not deny that the viruses from Wuhan were also among those.
However, the test seemingly also measures earlier SARS variants that are constantly altering, can change hosts quickly and are not found in virologists' databases. However, these were and are obviously not considered to be extraordinarily dangerous.
So how do we know that the discrepancy between the many harmless infections and the few more severe courses is not due to the fact that different variants are found equally well with the test used? Especially since it turns out positive even for animal variants!
However, a positive – although possibly meaningless – test result is always frightening and causes an immediate and predictable respective behaviour on the part of those affected and those responsible. The widespread testing, the fixation on ventilation problems, the emptying of the clinics for the announced flood of Covid-19 victims and triage exercises caused panic and thus guaranteed the obedience of a strongly intimidated population.
How to make fear last
When it became increasingly clear – even before the lockdown measures – that Germany would probably be mostly spared, two new foreign images of horror dominated the reporting in our country and ensured that fear and obedience continued: coffins and deadly chaos in many Italian and Spanish hospitals, refrigerated containers full of corpses and mass graves in New York. The conclusion was, that it had to be a dangerous epidemic after all.
However, it is unlikely that the same virus is so much more harmless in Hamburg than in New York. There must be other reasons for this.
Therefore I focused my research on these new focal points of the recent development. Perhaps, I hoped, it would then be easier to understand why many governments keep talking about the threat of a "second wave" and the continued need for a lockdown.
It is currently reasoned that the measures should be maintained more or less until the entire population can be saved by vaccination. One and a half years of a "new normality" without holidays, celebrations, cultural and sporting events are demanded and compulsory vaccinations, compulsory tests, tracking and immunity apps are held in prospect.
But why? How can the government be so sure to consider it necessary to repeal essential parts of the Basic Law, to drive the middle class into bankruptcy and to let workers and employees fall into unemployment? What else are we facing?
Medical Detectives: A look beneath the surface
The challenge is to find out what happened, for example, in Northern Italy, Spain or New York. In order to grasp this more research is needed, than what is taught in normal epidemiology. In Baltimore, at the now unfortunately institutionally corrupted Johns Hopkins University, I used to attend intensive epidemiological training, which gave me a great deal of methodological knowledge. There was also a branch called "Medical Detectives".
Here one could learn from history and on the basis of numerous well-researched cases how health consequences can arise, for example, from well or food poisoning and which tricks make it difficult to distinguish natural from man-made or even criminal causes. Medical detectives – everyone knows it from crime novels – have perpetrators and victims, motives and murder weapons, alibis and clients.
A disease – even one declared by the WHO – can be a "fake". In the cases of bird flu and swine flu, I have seen and investigated the unscrupulous and corrupt machinations of a pharmaceutical and vaccine industry. Time and again health fears have been created to divert billions of public money into private pockets with dangerous products.
That is why one may also ask about Covid-19: Could there be something else behind the public's continued anxiety? Qui bono? Who benefits from the fear?
Virologists once again as fear-mongers
Besides the WHO, the fear-mongers are again some virologists I already know from the past. Most of them – and this is unfortunately already "new normality" everywhere at medical institutes today – have established close cooperation with the pharmaceutical industry or other investors.
Nowadays it is easier to become a professor if you have shown skills in obtaining third-party funds. Science has become accustomed to "cheating", and the universities make this easier through non-transparent spin-offs, public-private partnerships or cooperation with alleged charitable foundations.
The virology department of the Berlin Charité is supported by the Bill and Melinda Gates Foundation regarding Covid-19. A co-author of the PCR test by Drosten et al. is the CEO of the biotech company TIB Molbiol, which is now increasingly producing tests and selling them for millions. However, these are detective secondary findings that do not explain by far what is turning this world upside down.
The majority of experts can no longer deny that the danger of infections in Germany and its neighbouring countries has already passed, without embarrassing themselves for the rest of their careers. And yet there are people in governments, public offices and the scientific community who want to lock us up with fear and keep on patronizing us.
My annoyance about this medically incomprehensible panicmongering and about many epidemic-hygienically nonsensical authorizations and freedom-withdrawing disciplinary measures is also accompanied by the curiosity of a "medical detective" who is concerned about possible hidden motives. Nevertheless, I do not want to deal with the political or economic background at this point. The time for this will probably come eventually. Moreover it is not my area of expertise.
Are we facing a "second wave"?
The question I ask myself is: How was it possible to create such horror scenarios with an apparently relatively harmless pathogen, whereby critics could be effortlessly eliminated and the fear in the population could constantly be fed by the media?
I would also like to know based on what scientific evidence the German Chancellor, her Minister of Health, her “virologist of choice” and others continue to announce: The second wave is yet to come. It will take many more months. We must not go on holiday. We have to be prepared to work from home in the future. We all have to be tested, tracked and vaccinated with a drug that has yet to be tested. Although all this is already laid out in the script with the title "The first modern pandemic", published by Bill Gates on April 23, it is not medically explained there either.
A hint from New York
On March 31 I received an important tip: New York intensive care physician Dr. Cameron Kyle-Sidell had alerted his colleagues with an astonishing observation. He reported:
"The Patients I saw in my ICU, they were no Covid-19 patients. They didn't have any signs of pneumonia, but rather looked like passengers on a plane, that suddenly lost pressure at high altitude."
Therefore It had to be a disturbance of the oxygen transport in the blood. I researched and ticked off the various known causes of such symptoms one after the other, if they were out of the question because of the progression of the disease. The most probable cause seemed to be rapid hemolysis, a destruction of the erythrocytes (red blood cells) that exchange oxygen in the lungs for Co2 to exhale in order to transport the oxygen to every corner of our body. Patients then feel suffocated, breathe very quickly and under great effort.
We know what to do in such a case because it is demonstrated to us in the aircraft before every take-off: Oxygen masks fall from the ceiling and bring relief until everything is back to normal. This is exactly what helped the patients in New York the best. Intubation and ventilation, on the other hand, were wrong and killed people in many places.
The Nigerian dead in Sweden
I was aware of such a case with the same puzzling symptoms, which had been described in 2014 by Swedish pneumologists in a young patient from Nigeria who had died of the disease. At that time, an enzyme deficiency was suspected and actually found to be a possible cause after death, which occurs in many regions of Africa in 20 - 30% of the population.
It is the so-called glucose-6-dehydrogenase deficiency, or "G6PD deficiency", one of the most common genetic peculiarities, which can lead to threatening haemolysis (dissolution of red blood cells), mainly in men, when certain drugs or chemicals are taken. The following map shows the distribution of this deficiency (Source and explanations here).
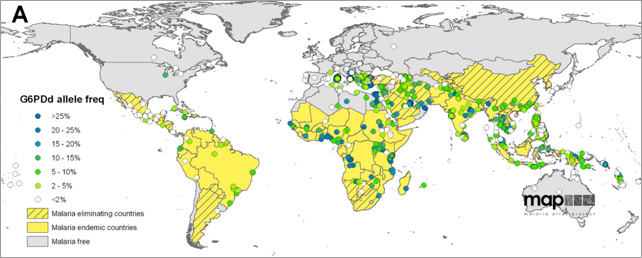
This hereditary trait is particularly common among ethnic groups living in areas with malaria. The modified G6PD gene offers advantages in the tropics. It makes its carriers resistant to malaria pathogens. However, G6PD deficiency is also dangerous if those affected come into contact with certain substances found in, for example, field beans, currants, peas and a number of medicines.
These include acetylsalicylic acid, metamizole, sulfonamides, vitamin K, naphthalene, aniline, malaria drugs and nitrofurans. The G6PD deficiency then leads to a disruption of the biochemical processes in the red blood cells and – depending on the dose – to mild to life-threatening haemolysis. The debris of the burst erythrocytes subsequently leads to microemboli, which block small vessels throughout the organs. What had caused the illness and death of the young man from Nigeria remained unclear at the time.
An alarming discovery
I looked at the drugs that can cause severe hemolysis in G6PD deficiency and got really scared. One of the substances that is called very dangerous in all forms of this enzyme deficiency is the anti-malarial drug hydroxychloroquine (HCQ).
But this is precisely the substance that Chinese researchers in Wuhan have been recommending against SARS since 2003. Along with the virus from Wuhan, HCQ now came back to us as one of the therapeutic options and was accepted as such. At the same time, HCQ was recommended as a promising agent against Covid-19 for further clinical trials with the support of WHO and other agencies.
According to reports, production of this drug is to be increased in Cameroon, Nigeria and other African countries. India is the largest producer of HCQ and exports it to 55 countries. Werner Baumann, Chairman of the Board of Management of Bayer AG, announced at the beginning of April that "various investigations in laboratories and clinics" had provided first indications that chloroquine might be suitable for the treatment of corona patients. The company then provided several million tablets.
There are now hundreds of trials worldwide, planned or ongoing by different sponsors, in which HCQ is used alone or together with other drugs. When I looked at some large studies to see if patients with G6PD deficiency were excluded, I found no evidence of this in most study plans. In the USA, for example, a large multi-center study with 4,000 volunteers from healthy medical staff is being prepared. Here, however, the term "hypersensitivity" is only used in general terms, as is the case with all drugs with regard to allergic reactions. In a chloroquine/hydroxychloroquine study by Oxford University (NCT04303507) with a planned 40,000 participants, the risk of G6PD deficiency is also not mentioned. In another large study by the Pentagon, though, there is an explicit warning to exclude G6PD deficiency patients from the study.
The following graph, based on information from the WHO database, shows how many studies on Covid-19 and HCQ have been initiated – and how few of them take enzyme deficiency into account.
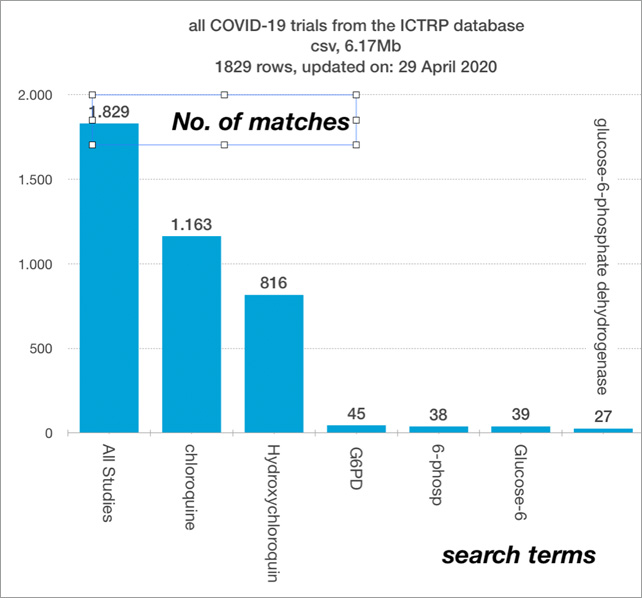
Mostly only the cardiac complications of chloroquine or hydroxychloroquine are mentioned, which in Brazil led to the premature termination of a study with 11 deaths of 81 subjects. However, it seems that worldwide little attention is paid to this further serious side effect. In addition, due to the lack of alternatives, HCQ has been tolerated and massively applied in many countries since the beginning of the year as part of a so-called "compassionate use". In medicine, compassionate use refers to the use of not yet approved drugs in emergency situations.
Conspicuous clusters
During this research, more and more results of more precise evaluations of the deaths in especially affected cities were received. In New York and other cities in the USA, it was reported that the vast majority of fatalities were African Americans – twice as many as could be expected based on the proportion of the population.
Also from England, where the mortality data from Euromomo shows an increasing death rate since the beginning of April, it was reported that 35% of about 2000 seriously ill people, twice as many as expected, came from ethnic "minorities" ("black, Asian or other ethnic minority"), including doctors and medical staff.
A major doctor's death in Italy remains in urgent need of clarification. The death of about 150 doctors and only a few female doctors is associated with Covid-19. Although age may have played a role in many of these cases, it should be noted that a high prevalence of G6PD deficiency has also been described for some regions of Italy and that in Italy up to 71% of those who tested positive with PCR, as well as the staff, had a prophylactic high level of HCQ. The same applies to Spain. Among the first 15 Covid-19 deaths in Sweden, there were 6 younger migrants from Somalia.
Deadly combination
Therefore the frightening result of my research is that typical severe courses with haemolysis, microthrombi and shortness of breath without typical signs of pneumonia occur more frequently where two factors come together:
- Many patients with ancestors from malaria countries with G6PD deficiency
- Prophylactic or therapeutic use of high-dose HCQ
This is exactly what is to be expected in Africa, and this is already the case everywhere where migration is causing a large proportion of the population coming from malaria countries. The following diagram shows the process flow schematically.
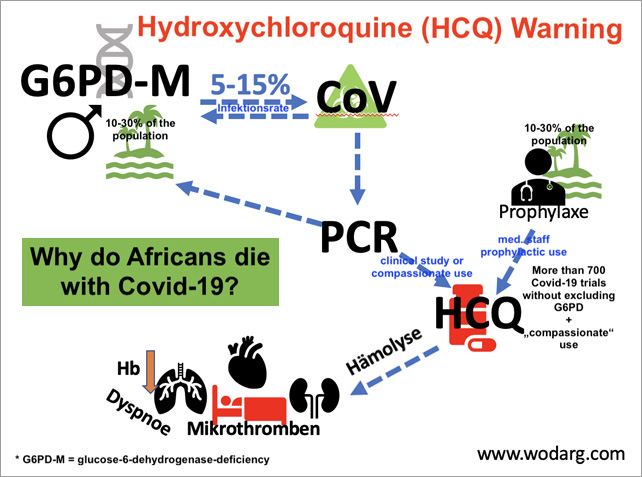
Cities such as New York, Chicago, New Orleans, London, or even large cities in Holland, Belgium, Spain and France are such centers. If the test is widely used in these migration hotspots and is expected to be positive in about 10 to 20% of the population, many people from the G6PD countries will also be among them. If they are then treated with high-dose HCQ, either prophylactically or as part of a "compassionate" use, as planned, then those severe clinical pictures will also be evoked in young people, as has been presented to us by the sensational press, and which keep our fear of Covid-19 alive.
It is unknown how many times this deadly combination has already led to victims. There has been no discussion of the issue among those responsible in the WHO and in governments. There is also a frightening lack of knowledge and sense of responsibility among doctors who are accountable for the treatment of Covid-19 patients or for the staff treating them.
Once again: This connection applies not only to Africa, but also to large parts of Asia, South and Central America, Arabia and the Mediterranean region.
However, the cases mentioned have nothing to do with Covid-19 disease. A PCR test result leading to the prophylactic prescription of HCQ is sufficient to cause severe disease in up to one third of the people from high-risk populations treated in this way.
HCQ treatment for G6PD deficiency is a dangerous malpractice
This could be remedied immediately if all treating physicians worldwide were informed about the contraindication of HCQ. However, the WHO, the CDC, the ECDC, the Chinese SARS specialists, the medical associations, the drug authorities and the German government and its advisors are carelessly neglecting to inform the public. In view of the ongoing programmes, this appears to be gross negligence.
It is a malpractice to treat people with G6PD deficiency with high-dose chloroquine derivatives or other drugs known to be dangerous for them. Under the WHO label "'Solidarity' clinical trial for COVID-19 treatments", healthy people are exposed in a hurry to authorised, life-threatening experiments. Hundreds of clinical trials, mostly worthless observational studies with parallel approaches, very often also run with HCQ as one of the alternatives.
German drug legislation prohibits the use of unauthorised drugs, but the government still encourages this. A non-validated test that is not approved for diagnostic purposes provides the pretext for the use of life-threatening medication – given an infectious disease where there is still no evidence that it poses serious risks beyond the risk of the annual flu epidemic.
At full throttle into the catastrophe
The dangers of this epidemic are presented with the help of scientific imposture. An unsuitable test from Berlin provides the pretext for deadly measures all over the world. The consequences of these mistakes lead to emergencies in many regions, which are attributed to an epidemic. This creates precisely the wave of fear so many in business and politics are now riding and which threatens to bury our fundamental rights.
The public, the media and the medical community hardly seem to be surprised that in New York and other centres more than twice as many "African Americans" die as would be expected due to their population share. Even in the studies of deaths in the USA and elsewhere, the risk posed by G6PD deficiency is almost always ignored or forgotten.
When sought-after virologists and other experts have been announcing for a long time that there will be a wave of deaths and terrible conditions in the cities in Africa, do they know about these connections? Or are there other provable reasons that justify such momentous prophecies? Finally: Is all this just a matter for science or also for public prosecutors and courts?
Note from the editor: Further information and graphics can be found on the author's website.
About the author: Dr. med. Wolfgang Wodarg, born in 1947, is an internist and pulmonary physician, specialist for hygiene and environmental medicine as well as for public health and social medicine. After his clinical activity as an internist, he was, among other things, a public health officer in Schleswig-Holstein, Germany for 13 years, at the same time lecturer at universities and technical colleges and chairman of the expert committee for health-related environmental protection at the Schleswig-Holstein Medical Association; in 1991 he received a scholarship at the Johns Hopkins University, Baltimore, USA (epidemiology).
As a member of the German Federal Parliament from 1994 to 2009, he was initiator and speaker in the Enquête Commission "Ethics and Law of Modern Medicine", member of the Parliamentary Assembly of the Council of Europe, where he was chairman of the Subcommittee on Health and deputy chairman of the Committee on Culture, Education and Science. In 2009, he initiated the Committee of Inquiry into WHO's role in H1N1 (swine flu) in Strasbourg, where he remained as a scientific expert after leaving Parliament. Since 2011 he has been working as a freelance university lecturer, doctor and health scientist and was a volunteer member of the board and head of the health working group at Transparency International Germany until 2020.


Diskussion
0 Kommentare